You would think that lasik would just be lasik. But, Whoa! Life can't be THAT simple. In fairness, much of the different types of lasik exist because lasik has been around for nearly three decades. And just how there are different types of phones (such as iphones, androids and even going back to flip-phones), lasik has evolved into different types as well.
Modern lasik takes advantage of the femtosecond laser to create the lasik flap. This is contrast to older types of lasik that use a blade. Different treatment methods exist to perform the prescription correction. These are known as wavefront-optimized, wavefront-guided and the newest and perhaps the most optimal, topography-guided treatments.
There are two main parts to lasik:
- The creation of the lasik flap
- The actual prescription treatment
Let's look at the distinct types of lasik for those two steps.
Different ways to create lasik flap
Lasik treatments are performed in the structural framework part of the cornea called the stroma. However, this stroma is covered by another layer on top called epithelium. We could brush off that epithelium to get down to the stroma for a treatment, but that would be called a different procedure - photorefractive keratectomy or PRK for short. Lasik does something different, it creates a window or flap to expose the stroma for treatment; compared to PRK, this improves the recovery time for lasik.
Microkeratome lasik (the type using blades)
Back in the day, lasik flaps were created using blades - called a microkeratome. While it sounds dangerous, microkeratomes weren't terrible. (after-all, if they were terrible, lasik wouldn't have caught on as a great way to correct vision).
Popular microkeratomes include the Moria microkeratome and the Hansatome microkeratome.
The instrument was calibrated to cut at a certain depth across the cornea. This created a regular two-dimensional cut within the cornea - creating a flap.
The advantage of the microkeratome is that it is cheap. Compared to lasers (which we'll get to in a second), the surgeon buys the microkeratome once and doesn't have to pay any additional costs to the manufacturer to use it.
Femtosecond lasik (the type using all lasers)
As technology improved, femtosecond lasers were developed which could create the lasik flap. Each pulse of this laser creates a microscopic air bubble pocket. These pockets are placed immediately adjacent to each other in the shape of a lasik flap. Following the treatment, the surgeon manually divides the final remaining connection between the tiny pockets to fold back the lasik flap for the treatment.
Popular femtosecond laser platforms for lasik include the iFS Intralase by Johnson & Johnson, the Wavelight FS200 by Alcon and the FEMTO LDV by Ziemer
Laser created lasik flaps offer significant advantages over microkeratomes (even despite the fact that each laser treatment has an additional cost, called a “click fee" that goes to the manufacturer).
- Laser created lasik flaps are much more secure and stable on the eye.
- The femtosecond laser is capable of creating complex geometries to the lasik flap. While a lasik flap doesn't need to be super complex, this does mean that the flap can be created in three-dimensions. Not only is a lasik flap bed created, but the flap is created with walls as well to sit better in place on the cornea. These walls can also be made with bevels to provide even more support and lock the flap in place.
- Using a laser will also create a small amount of inflammation at the edges of the lasik flap. This inflammation is a good thing - it adds just a little more microscopic scarring at the edge of the lasik flap. Scarring makes things stronger.
- Lasers can be more consistent.
- One issue with microkeratomes is that the blade can cut irregularly on certain corneas. This led to situations where the lasik flap was sliced cleanly from the cornea - called a free cap or other situations where there was a hold in the lasik flap - called a buttonhole. If these weren't managed properly, this could cause loss of vision. Femtosecond laser flaps thankfully don't have this issue.
- To avoid those irregular cut issues, microkeratomes often cut at deeper depths in the cornea. When talking about performing safe lasik treatments, depth matters. The deeper you go into the cornea, the less treatment you can safely perform. Because laser created lasik flaps are so consistent, they can be created at shallower depths of the cornea.
The addition of femtosecond lasers dramatically changed lasik and is very much worth the small extra cost that goes back to the manufacturer. (supporting future innovation perhaps?)
Different Ways To Perform The Lasik Treatment
Here's where things can get a little more confusing. There are multiple different technologies that are all competing to perform the best treatment. Unlike laser vs blade (which hopefully you've reached a clear conclusion), the uniform consensus on which is the best laser platform is a little more murky. Hint: all the most modern ways of doing a lasik correction work very good; but some do perform slightly better than others.
Here's what we'll cover:
- Conventional
- Wavefront-optimized
- Wavefront-guided
- Topography-guided
But first, a background on how lasik works
The prescription treatment during lasik is performed with an excimer laser. Each pulse of this laser shines on the stroma and is designed to remove microns of cornea tissue. The goal of all this is to change the shape of the cornea.
The cornea is responsible for approximately 2/3 of the prescription of the eye. For someone who is nearsighted, light doesn't focus properly on the retina. In particular, light focuses in front of their retina; their cornea bends and focuses light too much.
By flattening the cornea of someone who is nearsighted, light won't focus as much and will reach the retina completely in focus.
Thus, for nearsighted individuals, these laser pulses from the lasik laser are focused in the center of the cornea. Removing tissue from the center of the cornea causes that area to flatten.
Conventional
Let's start with conventional. This isn't considered one of the modern ways of doing lasik. This was the original way lasik treatments were performed.
Like the exact description on how lasik works, these lasers used very broad beams of excimer laser energy to flatten the center of the cornea.
But conventional treatments weren't perfect. You see, the cornea exists on a curve, like a dome. Energy from the laser that hit the sides of the dome wasn't the same as the energy that hit the center of the dome. This created large differences in treatment between the center of the cornea and the peripheral parts of the cornea. The periphery of the cornea remained steeper and focused light at a different location that the center treated part of the cornea. This led to an increase in something called spherical aberration - this causes halos and worse night time vision.
But even despite that, conventional lasik treatments were revolutionary for the time.
Why would some still perform conventional treatments? Well, for one, lasik lasers are expensive. If the practice doesn't do a high enough volume of lasik, then economically it may not make sense to upgrade to a modern version. In addition, similar to how the femtosecond laser has a "click fee" that goes to the manufacturer for each use of the laser, all modern lasers have these extra fees as well. But some of the older conventional lasik lasers existed before this trend began and thus lasik treatments can be performed at a lower cost.
Wavefront-optimized
How can we improve upon conventional treatments? Well, keeping the cornea more uniform would help. This is what wavefront-optimized treatments are designed to do.
The center of the cornea is treated as usual. This is called the optical zone - the part which you look through. But the peripheral cornea is also treated as well. Algorithms in the laser account for the slope of the peripheral cornea and apply more laser pulses to blend the peripheral cornea into the optical zone; reducing the large difference between peripheral and central cornea. This reduces the amount of spherical aberration to reduce halos and improve vision.
The Wavelight Allegretto Eye-Q introduced in the United States in 2006 and later replaced by the Wavelight EX500 in 2016 are some of the popular lasik lasers using wavefront-optimized treatments.
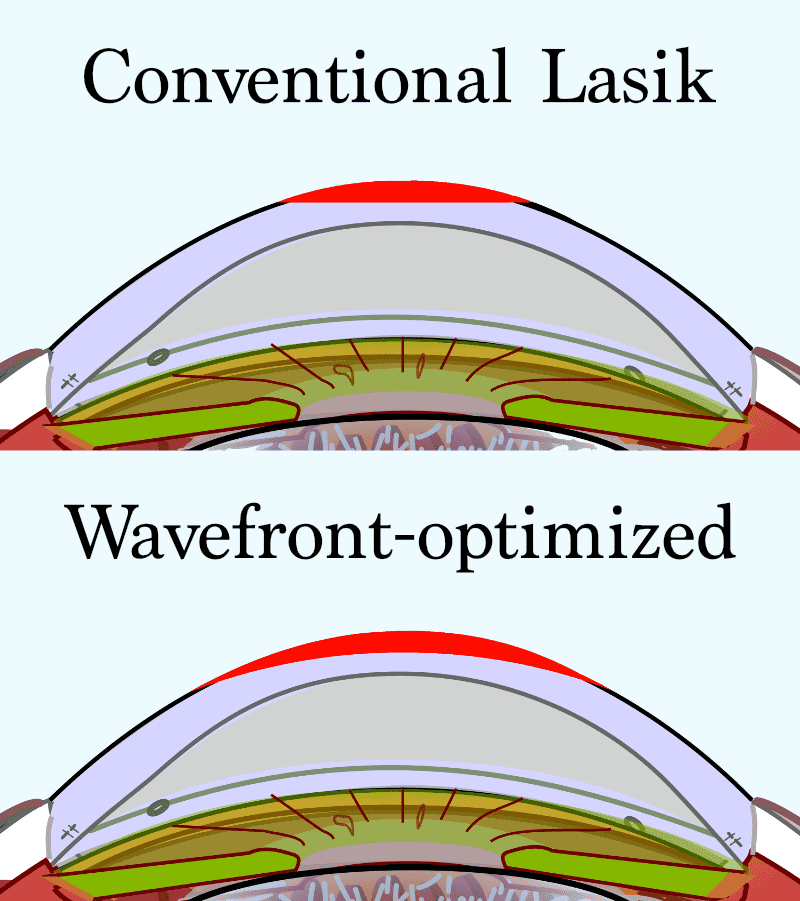
Conventional vs Wavefront-optimized Lasik; cornea graphic courtesy of Jmarchn, CC BY-SA 3.0, via Wikimedia Commons
{kind=link}
Wavefront-guided
Some laser manufacturers took a different strategy to correct vision and reduce the spherical aberration induced by conventional lasik. (and even attempt to reduce even more distortions in vision). This led to the development of wavefront-guided treatments.
Prior to lasik, the eye is measured with a special machine called an aberrometer. This machine shines light into the eye and measures its return after the light bounces off the retina in the back of the eye. This can measure the prescription of the eye and also measure extra distortions, called higher order aberrations in vision.
Aside to learn about higher order aberrations:
- When we correct our vision with glasses or contact lenses, we correct our spherical prescription (how nearsighted we are) as well as our astigmatism. Sphere and astigmatism are called lower order aberrations; those can be corrected with glasses because they have a simple symmetric and regular pattern. But there are also higher order aberrations which can blur vision. Because these don't have a simple pattern, glasses can't correct for these. Important higher order aberrations include our ole nemesis spherical aberration as well as something called coma and trefoil.
Wavefront-guided treatments take all this visual information from the aberrometer and uses it to calculate a treatment to correct not only the prescription, but also the higher order aberrations in the eye as well. Thus, it can treat things which glasses can't even treat.
The VISX Star S4 IR is a popular wavefront-guided treatment laser.
Unlike wavefront-optimized treatments, wavefront-guided treatments require an aberrometer. The VISX WaveScan CustomVue received FDA approval in 2005 which has since been improved to the iDESIGN in 2019
Topography-guided
So we have one type of lasik which focuses on creating a smooth blended treatment (wavefront-optimized) and another which focuses on reducing all sorts of distortions or aberrations in vision (wavefront-guided). Can both be done?
Many aberrations in our eye come from our cornea ie, the part of the eye that lasik actually treats. Some parts of the cornea may be slightly steeper than other parts of the cornea. This leads to a small amount of asymmetry.
The cornea can be mapped out - this is called topography. This map can tell us not only how much astigmatism there is on the cornea but also what higher order aberrations are coming from the cornea.
Once we have a map of the cornea, we can program the laser correction to eliminate the asymmetry in the cornea to correct corneal higher order aberrations at the same time as correcting prescription. Again, like wavefront-guided treatments, potentially improving vision from what glasses can do.
Contoura is a popular method for topography-guided treatments in the United States and became available in 2015.
Contoura is used with the EX500 laser. Sound familiar? This is the same laser used for wavefront-optimized treatments. The same laser can be programmed for Contoura topography-guided treatments (with an additional “click fee" cost above the normal one to the manufacturer, of coure; and also as long as cornea measurements were performed by the Wavelight Vario Topolyzer topography machine prior).
But because the EX500 is used, wavefront-optimized principles are applied to the topography-guided treatment to create as smooth of cornea as needed for optimal vision.
So Which Is Best?
In reality you can't go wrong with either of the modern lasik treatments. Wavefront-optimized, wavefront-guided, and topography-guided treatments all work very similarly to correct vision. (in fact, visiting an experienced lasik surgeon may make a bigger difference in outcome).
But of course, you want to know the best!
Wavefront-optimized vs wavefront-guided
For the longest time, there really wasn't any significant difference in outcome between wavefront-optimized treatments and wavefront-guided treatments. Despite wavefront-guided treatments targeting extra aberrations in the eye, both treatments had very similar outcomes. No significant change in vision results.
However, the aberrometer machine used for wavefront-guided treatments became more advanced. This allowed the aberrometer to measure the eye better than the older technology. And this actually changed outcomes!
While the vision acuity (the ability to read letters on an eye chart) between the two treatments was still the same, the upgraded machine allowed wavefront-guided treatments to have slightly better ability to see differences in shades of light and dark, known as contrast sensitivity. This can potentially improve vision in low light scenarios. Still very similar but a slight edge to wavefront-guided treatments.
Wavefront-guided vs topography-guided
Here's where things get a little more murky. For one, direct comparisons between wavefront-guided and topography-guided treatments are more sparse. The second is that our understanding of the optimal way to use topography-guided treatments is increasing year by year.
The aberrations that we have on our cornea (the ones specially treated with topography-guided treatments) actually contribute to our overall prescription in subtle ways. Simply treating those aberrations without adjusting for changes in the prescription can reduce the accuracy of the treatment. Because of this, early topography-guided treatments weren't as accurate as wavefront-optimized and wavefront-guided treatments.
Starting in 2019, the Phorcides Analytical Engine was created to assess the impact these corneal aberrations have on prescription. Adjustments are made to the treated prescription in order to improve the accuracy of topography guided treatments. This has improved the ability of topography-guided treatments to provide sharper vision. After topography-guided lasik with Contoura and Phorcides, over a third of patients will see better without glasses than they ever saw with glasses.
Wavefront-guided lasik still works very well, but topography-guided lasik has the slight edge.
Conclusion
While there are clear differences in the type of lasik when it comes to the creation of the lasik flap, there is less dominance when it comes to the type of laser used to perform the actual prescription treatment. All things being equal, topography-guided lasik has the potential to perform slightly better than wavefront-guided and wavefront-optimized treatments. But either way, today's lasik works extremely well to correct your vision and get you out of glasses and contact lenses.
Lasik Marketing Term Cheat Sheet
- Custom Lasik - Technically should be used for wavefront-guided and topograpy-guided; but also sometimes used for wavefront-optimized (since the treatments are "customized" or adjusted based upon the curvature of the cornea)
- IntraLasik or iLasik - Lasik using the femtosecond intralase laser to create the lasik flap (it's a good laser)
- Z-Lasik - Lasik using the femtosecond ziemer laser to create the lasik flap (also a good laser)
- Ultra Lasik - Lasik using a femtosecond laser (which can create "ultra-thin" flaps, ie thinner flaps than microkeratome lasik)
- Lasek - Not lasik, a type of PRK using alcohol to remove the epithelium with an attempt to try to replace it
- Epi-Lasik - Also not lasik, another form of PRK using a different microkeratome to cut away the epithelium with an attempt to try to replace it
Like what you just read? Use Social Media?
Stay connected and join the discussion by following Eye Mountain on
Also Check Out: